Let's transform cardiovascular care together
If you are an employer or payer looking for a comprehensive heart health enterprise solution, contact us.
Our Technology
Our Solutions
For Life Sciences Industry
I've spent most of my professional life studying ECGs. If there's one thing I've learned, it's this:
Every time we think we've extracted all the information from the ECG, it surprises us.
A recent Nature paper reminded me of that once again.
Researchers developed an AI model that predicted sudden cardiac death more accurately than existing methods based on a reduced Ejection Fraction (EF). What caught my attention wasn't simply the performance of the model—it was how it achieved it. The investigators described a previously unrecognized ECG signature involving left axis deviation, poor R-wave progression, and subtle morphology in lead aVL.
For me, that's the real story.
It reminds us that the ECG still contains information we don't yet fully understand.
We spend a lot of time talking about better AI.
Perhaps we should spend just as much time talking about better signals.
A single-lead ECG has transformed ambulatory cardiac care and remains an incredibly valuable tool. But every additional lead provides another electrical perspective of the heart. More perspectives mean more information for physicians—and potentially more information for future AI models to discover.
The goal isn't to collect more data.
It's to preserve more of the heart's electrical story.
This principle is already relevant in everyday clinical practice.
Consider Wolff-Parkinson-White syndrome here revealed in Lead II only.
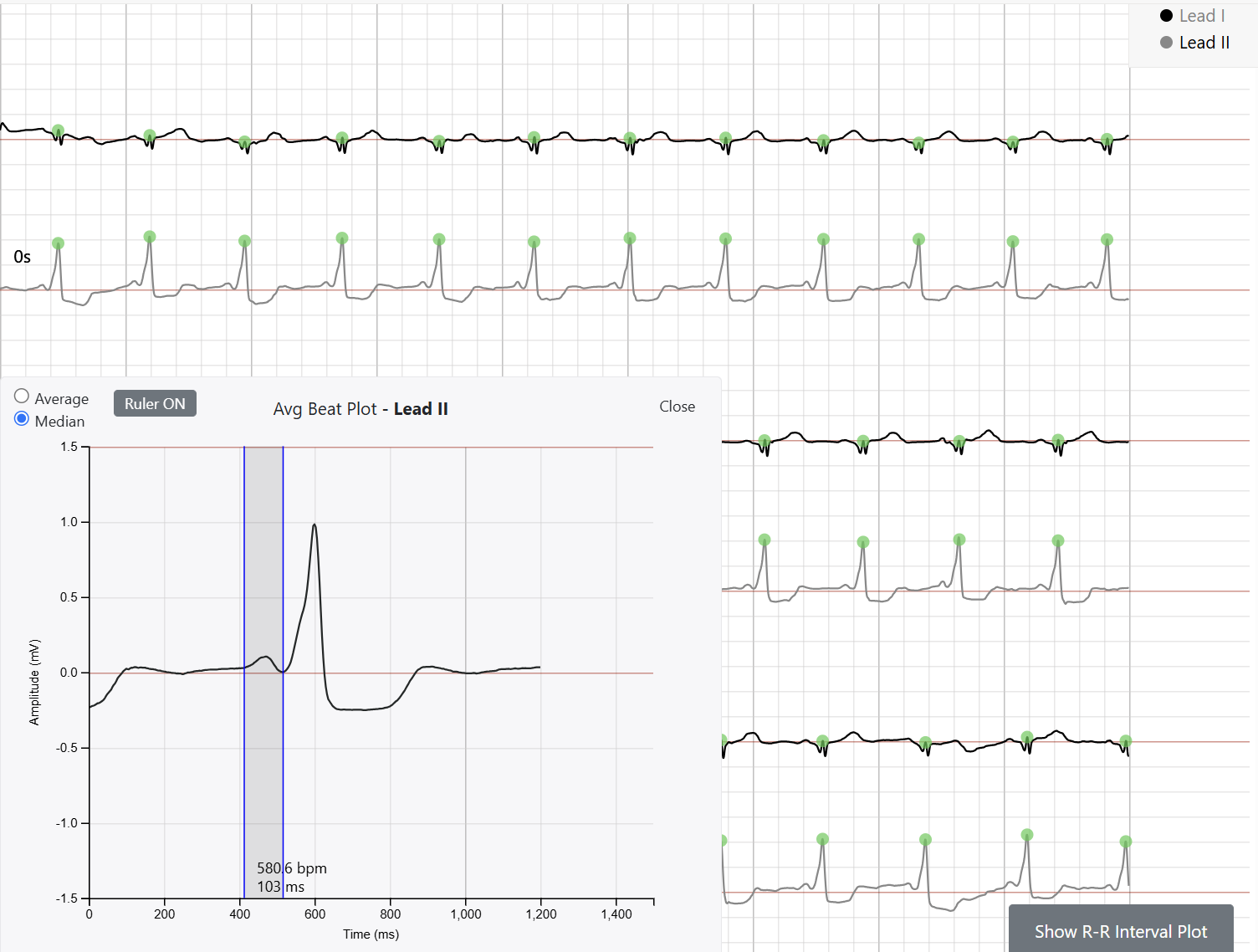
When the findings are classic, an experienced physician can often recognize ventricular pre-excitation from a single lead. But ambulatory ECGs aren't recorded in ideal conditions. Patients move. Electrodes shift. Motion artifact happens.
Having multiple simultaneous limb leads often means that when one lead is noisy, another provides a clearer view of the same heartbeat. That additional perspective can improve confidence when evaluating PR interval, delta wave morphology, electrical axis, and the overall pattern of ventricular activation.
It isn't about replacing physician expertise.
It's about giving physicians more information to work with.
That philosophy has guided our thinking from the beginning.
When we developed the KardiaMobile 6L Max, the objective wasn't simply to add more leads. It was to preserve more clinically useful information while keeping the device simple enough for patients to use anywhere.
By recording Leads I and II simultaneously and deriving the remaining frontal-plane limb leads, KardiaMobile 6L Max captures substantially more electrical information than a single-lead recording. That richer signal gives physicians additional context for rhythm interpretation, conduction abnormalities, electrical axis, ECG morphology, QT assessment, and other clinical observations within the device's intended use.
Just as importantly, patients can capture that information at the moment symptoms occur—whether they're at home, traveling, or awake at 2 a.m. with palpitations—rather than hoping those symptoms recur during an office visit.
For physicians, that's more information.
For patients, that's better access to meaningful cardiac evaluation.
The Nature paper does not establish a role for ambulatory ECG in predicting sudden cardiac death, nor does it change the intended use of KardiaMobile 6L Max.
What it does reinforce is a principle I've believed for many years.
The ECG remains one of medicine's richest physiological signals.
As cardiovascular science continues to evolve, new clinical applications will undoubtedly emerge. Some will come from AI. Others will come from physicians asking new questions of the data we already have.
Either way, discovery begins with the signal.
That's why I continue to believe that preserving more of the heart's electrical information—in a form patients can easily capture and physicians can meaningfully interpret—is one of the most important directions in ambulatory ECG.
After more than a century, the ECG is still teaching us. I suspect we're only beginning to understand what it has to say.
The research discussed above represents independent academic work and should not be interpreted as establishing a clinical indication for any AliveCor product. KardiaMobile 6L Max is FDA-cleared for detection of atrial fibrillation (AF), bradycardia, tachycardia, normal sinus rhythm, sinus rhythm with premature atrial contractions (PACs), sinus rhythm with premature ventricular contractions (PVCs), sinus rhythm with wide QRS, and QT interval assessment. AliveCor does not make claims regarding prediction of sudden cardiac death. Clinical decisions should always be based on a physician's comprehensive evaluation of the patient.
Let's transform cardiovascular care together
If you are an employer or payer looking for a comprehensive heart health enterprise solution, contact us.